
|
Patient Position
- Have the patient stand with their feet shoulder width apart with the plumb line located directly beside of them but not in contact. Directions - Assure that the plumb line lines up so that the lateral malleolus of the exposed legs sits just posterior to the plumb line. - Capture an image of the patient to use for analysis. Rules of the Analysis - Due to the uneven nature of the human body this aspect of the postural analysis should be performed bilaterally. Key Points of the Analysis - Knee - Observe the knee angulation and make note of any evidence of knee hyperextension while the patient is in a comfortable stance. - Spine - Observe the spine from a lateral view and make note of any curvature observed in the spine. - Shoulders - Observe the location of the acromion process. Make note of any presence of the acromion process that is anterior to the plumb line. - Skull - Observe the skull position in relation to the plumb line. The plumb line should run so that it touches the posterior portion of the ear. Make a note of any deviation from this condition. |
Implications and Rehabilitation Direction
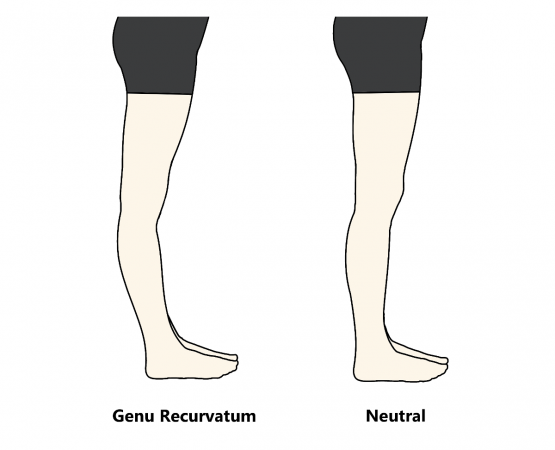
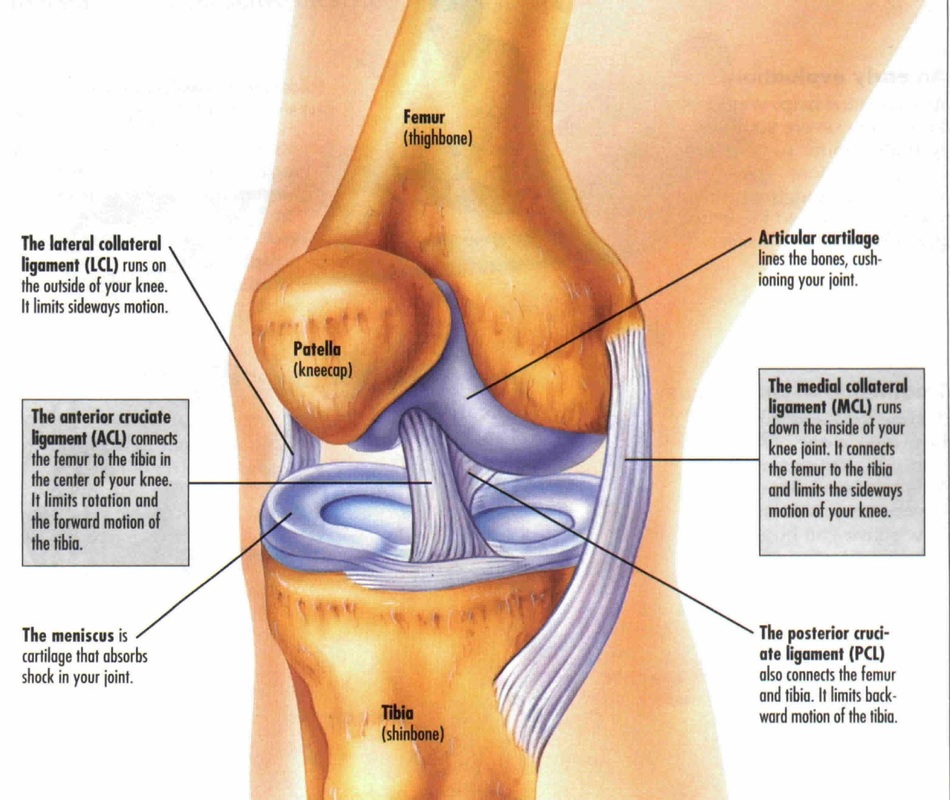
- Knee - When knee hyperextension is present from this view it indicates the patient has genu recurvatum (graphic below (left)). This is a condition where the angle of knee flexion is less than 0. This condition is benign in most patients but does predispose you to injuries of the ligaments of the knee joint as well as the meniscus (structures in graphic below (right)).
- Knee - When knee hyperextension is present from this view it indicates the patient has genu recurvatum (graphic below (left)). This is a condition where the angle of knee flexion is less than 0. This condition is benign in most patients but does predispose you to injuries of the ligaments of the knee joint as well as the meniscus (structures in graphic below (right)).
|
|
Genu recurvatum is treated with aggressive prescription rehabilitation exercises. A rehabilitation program for an individual with this condition should focus on strengthening the posterior muscles of the leg. These muscles include the hamstring muscles (biceps femoris, semitendonosus & semimembranosus) and the calf muscles (gastrocnemius and soleus). For details of the hamstring muscles refer to the 90-90 test page of this website. The calf muscles are shown below. Strengthening these muscles will create tighter muscles and in turn increase the angle of knee flexion.

|
The primary movement the calf muscles are responsible for is resisted plantar flexion. The gastrocnemius is the primary muscle when plantar flexion is performed while knees are straight. The soleus is the primary muscle when plantar flexion is performed while knees are bent. |
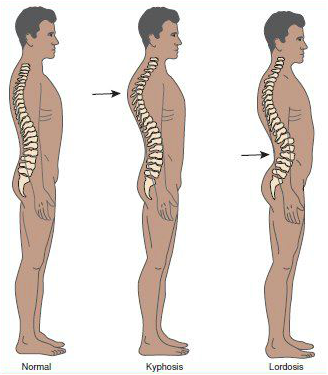
- Spine - There should be a normal curve present in the spine upon examination. Extreme posterior curvature of the thoracic vertebrae is a condition called kyphosis and is usually found in tandem with a posterior tilt of the pelvic bone. Extreme anterior curvature of the lumbar vertebrae is a condition called lordosis and is usually found in tandem with an anterior tilt of the pelvic bone. These conditions are usually both benign until they are older (30+ years of age) and begin to experience pain due to the degenerative conditions that arise from the constant stress placed on certain regions of the spine. Due to this negative prognosis and the pelvic tilt that will create postural problems throughout the body, a patient who has either condition should begin prescribed rehabilitation exercises as soon as it is found that they have either of these conditions. A rehabilitation program for a patient that presents with kyphosis or lordosis should include exercises that strengthen the interspinal muscles that run along the length of the spine. For a detailed look at the interspinal muscles refer to the posterior view page of this website.
|
Kyphosis - Extreme posterior curvature of the thoracic vertebrae. - This spinal alignment causes a posterior pelvic tilt. Lordosis - Extreme anterior curvature of the lumbar vertebrae. -This spinal alignment causes a anterior pelvic tilt |
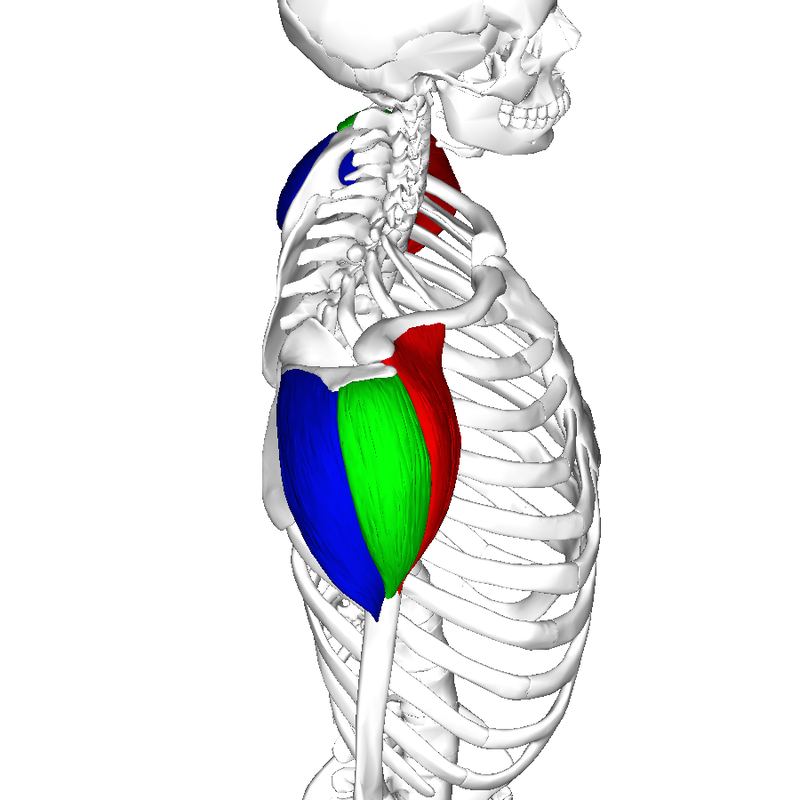
- Shoulders - The acromion process should be bisected by the plumb line. If the acromion process appears anterior to the plumb line it indicates tight anterior muscles of the chest and deltoid. A rehabilitation program for an individual with should include a stretching routine involving the pectoral muscles and anterior deltoid. The rehabilitation routine should also include strengthening exercises for the posterior and medial deltoid muscles. For a detailed look at the pectoral muscles refer to the pectoralis major/minor page of this website. The deltoid muscles are highlighted in the graphic below.
|
Anterior Deltoid (Red) - The anterior deltiod is the primary muscle responsible for shoulder flexion. The anterior deltoid also aids the pectoral muscles with horizontal adduction. Medial Deltoid (Green) - The medial deltoid is the primary muscle responsible for shoulder abduction. Posterior Deltoid (Blue) - The posterior deltoid is the primary muscle responsible for shoulder extension and works in tandem with the rhomboids for horizontal abduction. |
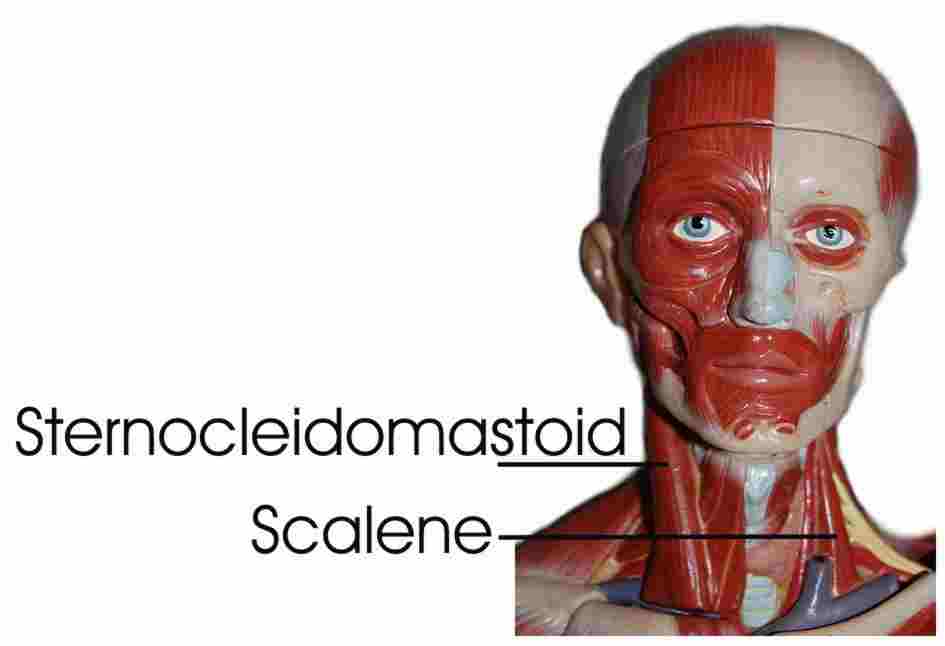
- Skull - The skull should be positioned so that the plumb line touches the posterior portion of the ear. If the ear sits forward of the plumb line it indicates tight sternocleidomastoid muscles and tight scalene muscles. This condition is also referred to as forward head posture. A rehabilitation program for a patient with this condition should involve stretching of the involved muscles (found in the images below)
|
Sternocleidomastoid Primary Actions - Cervical rotation - Cervical lateral flexion Scalenes Primary Actions - Elevation of the 1st and 2nd rib - Cervical lateral flexion |
